
|
Toll Free 1-800-998-9729 |
Home About Us Why Choose Us What We Do Track Record Client Quotes Questions? Mesothelioma FAQs Legal FAQs How We Can Help Asbestos Industry History Work Exposure Military Exposure Home Exposure Asbestos Products Asbestos News Case Evaluation |
Pulmonary Perspectives, September 2001 Volume 18, Issue 3Mesothelioma: An Emerging EpidemicThe incidence of malignant mesothelioma, a neoplastic process affecting the pleura, and to a lesser extent the peritoneum, is increasing. Mesothelioma is almost always caused by inhalation of asbestos fibers years before the development of the malignancy. Since asbestos exposure generally occurs on the job site, obtaining a thorough occupational history is critical. The elapsed time between first exposure to asbestos and the development of an asbestos-induced disease is called latency. The minimum latency for mesothelioma is 10 years; however, a latency of 30 to 40 years is more usual (Finnish Institute. Scan J Work Environ Health 1997; 23:311). Latency and longevity are key factors in the mesothelioma epidemic of 2000. EpidemiologyTwenty to forty percent of adult men report occupational exposure to asbestos (Finnish Institute. Scan J Work Environ Health 1997; 23:311). This reported range likely underestimates the true frequency of asbestos exposure because most workers are either unaware of or are unable to remember the nature of their exposure. An estimated 27 million workers were exposed to asbestos in the United States between 1940 and 1979 (Kamp and Weitzman. Soc Exp Biol Med 1997; 214:212). Even brief or low level exposure is sufficient to cause mesothelioma. One marker of asbestos exposure is the presence of pleural plaques on the chest radiograph. The National Health and Nutrition Examination Survey (NHANES) data reveal that 6.4% of men and 1.7% of women age 35 to 74 have a discernible pleural plaque (Kamp and Weitzman. Soc Exp Biol Med 1997; 214:12). 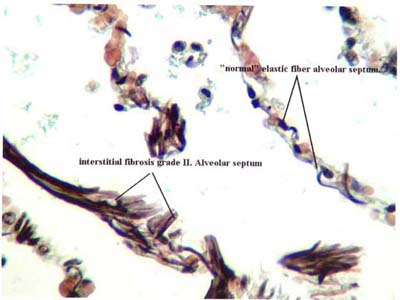 Magnified view of Grade II interstitial fibrosis in lung tissue. The prevalence of asbestos-related parenchymal and pleural abnormalities within an asbestos-exposed population increases with age. We have recently shown that 23% of asbestos-exposed workers previously found to be free of asbestos-induced lung disease showed pleural or parenchymal evidence of asbestos-induced lung disease when rescreened 10 years later (Liang et al. Am J Respir Crit Care Med 2001;163:A167). In the United States, the average retiree now has an extended life expectancy compared to previous generations. Compared to 2 decades ago, when the median collection time for pension checks was 17 months, the average life expectancy today of a man at the age of 65 is 81 or an average of 92 total pension checks. Consequently, it is anticipated that the prevalence of mesothelioma will increase. 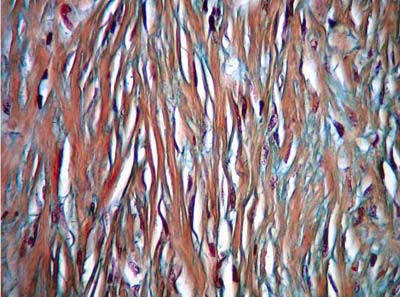 Magnified view of Grade II interstitial fibrosis in lung tissue. So, as the population ages and individual life expectancy is prolonged, the prevalence of mesothelioma is expected to increase as the long latency period is fully expressed. In Great Britain, the incidence of mesothelioma is expected to continue to increase over next 20 years (British Thoracic Society Standards of Care Committee. Thorax 2001; 56:250). The worst affected cohort to date in Britain is a man born in the 1940s. Mesothelioma may account for 1% of all deaths in this cohort. The peak incidence in Great Britain is projected for the year 2020, while the incidence in the United States may have already reached its apogee (Peto et al. Lancet 1995; 345:535). The projected peak incidence in the United States, for men older than 75 years of age exposed in the 1930s through the 1960s, was the year 2000 (Nishimura and Broaddus. Clin Chest Med 1998; 19:311). This projection fails to take into account, however, the increasing longevity experienced by this cohort as a direct consequence of medical advances primarily related to smoking cessation, minimally invasive management of coronary artery disease, blood pressure and cholesterol control measures, as well as early detection of prostate cancer. Work HistoryDespite therapeutic advances in the last decade (parietal pleurectomy, extrapleural pneumonectomy, combination chemotherapy, and gene therapy), the median survival for patients with mesothelioma remains 8 to14 months. Studies demonstrating improved survival in mesothelioma using these newer treatment modalities have uniformly recruited patients with early stage disease and excluded those with late stage disease. We have shown that most patients with mesothelioma are diagnosed at a late stage (251days after initial evaluation for symptoms), which accounts for the short survival after diagnosis despite advances in medical care. The primary cause of this delay in diagnosis is the lack of clinical suspicion of mesothelioma because of a failure to elicit a detailed occupational history. A thorough work history provides the most practical and useful measure of asbestos exposure (Finnish Institute. Scan J Work Environ Health 1997; 23:311). Jobs in construction and building maintenance are the most commonly related to asbestos exposure (Peto et al. Lancet 1995; 345:535). These occupations include pipe fitters, plumbers, welders, sheet metal workers, millwrights, lathers, painters, electricians, boilermakers, plasterers, and laborers. Demolition work is also a common source of exposure. Building materials that may contain asbestos include putties, caulk, firebrick, sheet rock (wallboard), shingles, siding, plaster, ceiling, and floor tiles, as well as insulation. Compounds used in industry that have contained asbestos include welding rods, gaskets, grinding wheels, refractory materials, and pump and valve packing. Women have frequently been exposed in the textile industry as machine operators, upholsterers, and also in glass works. Other exposure risk occupations include workers in refineries, foundries, paper mills, car and truck assembly lines, steel industries, munitions manufacturing plants, shipbuilding, naval services, chemical industries, carpentry, and railroad workers, especially engineers, brakemen, and firemen (even after the steam engine era). Clinical AspectsPatients generally present to their physician with complaints of dyspnea, chest pain, and pleural effusion. The chest radiograph often shows a pleural effusion or pleural thickening that is either nodular or asymmetric. Without the valuable knowledge of an asbestos exposure history, physicians waste precious time treating signs and symptoms of mesothelioma with antibiotics, diuretics, and repeated thoracenteses. Diagnostic thoracentesis that reveals a lymphocytic exudate in the setting of a positive exposure history should prompt early pleural biopsy. Closed pleural biopsy is 50% sensitive, and pleural fluid cytology has a sensitivity of 32%. Therefore, neither negative findings on pleural fluid cytology or pleural biopsy exclude the possibility of malignant mesothelioma. Biopsy can also be accomplished through video-assisted thoracoscopic surgery (VATS) with higher yields. At times, either because of dense pleural adhesions or the inability to sample adequate tissue, a full thoracotomy is required. Mesothelioma often invades the needle or biopsy tract. Mesothelioma cell types include epithelioid, sarcomatous, and biphasic. The epithelioid cell type is more common than other pathologic types and has the best prognosis. The differential diagnosis includes metastatic adenocarcinoma, fibrothorax from previous trauma, chronic organized empyema, and benign pleural thickening. Immunohistochemical staining aids in distinguishing metastatic adenocarcinoma from mesothelioma. Only 1 to 5% of mesothelioma cases are suitable for radical surgery such as pleurectomy or extrapleural pneumonectomy. Only patients with the epithelioid cell type should undergo radical surgery and only in highly specialized surgical centers. Even with well-chosen patients, the operative mortality of these procedures can be nearly 30%. Talc pleurodesis is the treatment of choice for the of control pleural fluid accumulation (British Thoracic Society Standards of Care Committee. Thorax 2001; 56:250). Prophylactic radiation therapy reduces chest wall implantation following invasive procedures. Palpable subcutaneous masses respond to radiation therapy in about half of all patients. Palliative radiation therapy provides pain relief in about half of all patients. There are no published randomized trials comparing either survival or symptom control in patients treated with chemotherapy vs best supportive care. Chemotherapy, when used, should be given as part of a clinical trial. Gene therapy, photodynamic therapy, and immunotherapy do not yet have an established role (British Thoracic Society Standards of Care Committee. Thorax 2001; 56:250). SummaryThe incidence of mesothelioma is increasing within this decade. Latency and longevity are key factors in this epidemic. The diagnosis of malignant mesothelioma should be considered in all patients with the potential for occupational exposure who present with complaints of dyspnea or chest pain and radiographic evidence of pleural effusion or asymmetric pleural thickening.
|
||
|